ACL Injuries in Adolescents: Understanding the Challenges and Treatment Options
Introduction: Anatomy, Prevalence, and High-Risk Sports
The anterior cruciate ligament (ACL) is a critical stabilizer of the knee joint, connecting the femur to the tibia and preventing excessive forward movement of the tibia. ACL injuries are among the most common knee injuries in active adolescents, particularly in high-risk sports such as soccer, basketball, football, and gymnastics. Studies show that the incidence of ACL injuries in young athletes has risen in recent years, coinciding with increased specialization in single sports and year-round training. A notable aspect of ACL injuries is their prevalence among female athletes. The increased risk of ACL ruptures in adolescent females, and females in general, is multifactorial and has been attributed to several factors. These include an increased Q-angle (the angle formed by the quadriceps muscle relative to the patella), increased knee valgus motion upon landing, and differences in neuromuscular control, hormone levels, and biomechanics. These factors collectively contribute to higher stress on the ACL during athletic activities such as jumping, landing, and cutting motions.
Treatment Options
Nonoperative management, such as physical therapy and bracing, is sometimes considered for less active adolescents. However, it often results in persistent knee instability and an inability to return to their preferred sports and activities. Furthermore, research has shown that delayed ACL surgery in this patient population is associated with a higher risk of secondary meniscus and cartilage injuries. These injuries can lead to early osteoarthritis, a condition linked to pain and decreased quality of life. Operative management, primarily ACL reconstruction, is preferred for active adolescents to minimize these risks and enable a safe return to sports, as untreated ACL injuries can negatively impact physical and psychological well-being (James et al., Am J Sports Med, 2021).
Growth Plate Considerations in Adolescents
Treating ACL injuries in adolescents requires a unique approach due to the presence of open growth plates, or physes. These growth plates are areas of cartilage at the ends of long bones, which allow for bone elongation during development. On average, girls’ growth plates close around age 14, while boys’ close around age 16. Significant growth remaining can complicate surgical decisions, as injuring the growth plates during surgery could lead to leg length discrepancies or angular deformities. When tailoring surgical options for adolescents with open growth plates, surgeons aim to preserve these structures. This involves choosing techniques that avoid drilling through the physes or applying stress to the growth plates.
Surgical Options for ACL Injuries in Adolescents
ACL Reconstruction
ACL reconstruction replaces the torn ligament with a graft, typically harvested from the patient’s own hamstring or quadriceps tendons. Graft harvesting involves removing a section of tendon from the patient’s body (autograft) to create a new ligament that restores knee stability and function. This procedure is considered the gold standard for adolescents and Adults with ACL injuries. Soft tissue autografts are preferred (hamstrings and quadriceps) because they minimize the risk of growth plate disturbances while providing a durable replacement for the torn ligament.
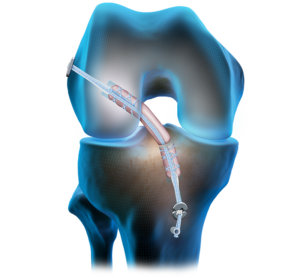
(ACL reconstruction)
Why Not Allografts?
Allografts, or grafts from deceased donors, offer the advantage of avoiding graft harvesting; however, they are generally avoided in this age group due to their higher failure rate, especially in young, active individuals. Studies show that allografts are more prone to re-tears compared to autografts in adolescents (Kaeding et al., Am J Sports Med, 2011).
ACL Repair
ACL repair involves stitching the torn ligament back together in an attempt to restore its original function. While this procedure avoids graft harvesting and can reduce recovery time, it is now rarely recommended in adolescents due to a high failure rate. The recurrence of injury has limited its use in this population (Vermeijden et al., Arthroscopy, 2021).

(ACL repair)
Growth Plate-Sensitive Techniques
Surgeons use growth plate-sparing techniques to minimize risk, such as extracortical fixation or placing tunnels away from the physes. In patients whose growth plates have closed, the surgical approach mirrors that of adults, allowing for more standard reconstruction techniques.

Recovery Timeline and Return to Sport
Rehabilitation after ACL reconstruction is a gradual process that focuses on restoring range of motion, strength, and functional stability. On average, recovery takes 9-12 months, with the goal of preparing the athlete for a safe return to sports. A systematic review and meta-analysis found that over 90% of children and adolescents return to sport after ACL reconstruction, highlighting the efficacy of surgical techniques and rehabilitation protocols (Kay et al., Knee Surg Sports Traumatol Arthrosc, 2018). However, readiness for return to sport depends on meeting specific milestones, including strength symmetry, neuromuscular control, and psychological readiness.
Conclusion
ACL injuries in adolescents pose unique challenges due to the presence of open growth plates and the demands of an active lifestyle. By tailoring surgical approaches to the patient’s growth and activity level, and by prioritizing proper rehabilitation, young athletes can achieve successful outcomes and return to the sports they love. If you or your child has experienced an ACL injury, consult with an orthopedic specialist to determine the most appropriate treatment plan. For more information on ACL injuries and treatment options, visit PaulRothenbergMD.com/acl-surgery.
References
- James E.W., Dawkins B.J., Schachne J.M., Ganley T.J., Kocher M.S., et al.; PLUTO Study Group, “Early Operative Versus Delayed Operative Versus Nonoperative Treatment of Pediatric and Adolescent Anterior Cruciate Ligament Injuries: A Systematic Review and Meta-analysis,” Am J Sports Med, 2021; 49(14):4008-4017.
- Vermeijden H.D., Yang X.A., van der List J.P., DiFelice G.S., “Role of Age on Success of Arthroscopic Primary Repair of Proximal Anterior Cruciate Ligament Tears,” Arthroscopy, 2021; 37:1194-1201.
- Kaeding C.C., Aros B., Pedroza A., “Allograft Versus Autograft Anterior Cruciate Ligament Reconstruction: Predictors of Failure,” Am J Sports Med, 2011.
- Kay J., Memon M., Marx R.G., Peterson D., Simunovic N., Ayeni O.R., “Over 90% of Children and Adolescents Return to Sport After Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-Analysis,” Knee Surg Sports Traumatol Arthrosc, 2018; 26(4):1019-1036.